How to Prevent Chronic Pain After Knee Replacement
Knee replacement is in large part an overwhelmingly successful procedure for millions of Americans each year, with as many as 86% of patients achieving a substantially meaningful improvement and success after surgery(1). However, as many as 10-20% of patients undergoing knee replacement may be unhappy with the results of their replacement, even when obvious issues, such as infection or loosening, are discounted. Many individuals may even know someone with a replacement that hurts or is a cause for dissatisfaction. What would make someone with a knee replacement that has “good” X-ray appearance, allows them to walk, and does not have evidence infection be unhappy? We explore some of the reasons for “aseptic” failure of knee replacements below.
Some of the causes of aseptic failure of a knee replacement include instability, malalignment, patellar (kneecap) maltracking, and stiffness. These are causes that are subtle, not easily identified on routine tests such as X-rays, which can generally pick up loosening of the implant.
Instability of the knee prosthesis is seen in nearly 24% of failed knee replacements, and is typically related to the primary implantation(2). Instability of the knee prosthesis frequently causes looseness with flexion of the knee, where the ligaments are balanced in extension but lax in flexion. This is demonstrated in the figure. One of the reasons this can happen exemplifies the pitfalls of a manually instrumented knee where the surgeon makes the standard preparations for placement of the femoral component of the knee, not realizing that an insufficient amount of bone from the end (distal part) of the femur has been removed. This leads to a tight implant and the only way to get the knee to straighten is to use a thin liner, balancing the knee in extension but leaving it loose in flexion.
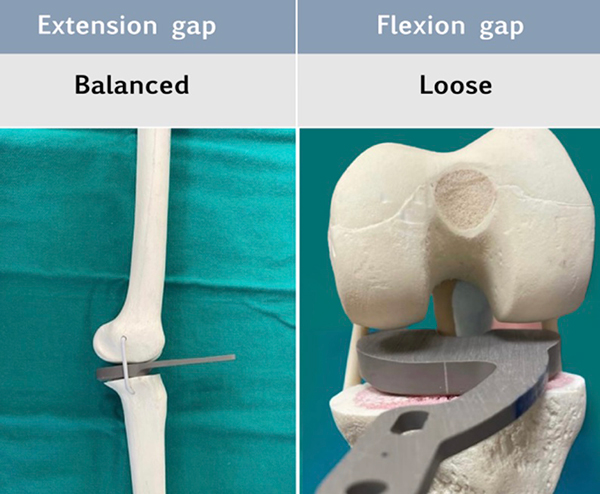
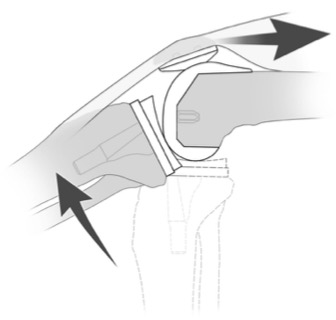
Flexion instability leads to pain when “starting up” or rising from a seated position, pain with stairs, and difficulty with uneven surfaces. The reason for these symptoms relates to the additional work the extensor mechanism must generate to pull the tibia up into contact with the femur to effectuate knee extension. Usually this is usually an efficient process but can be complicated and ineffective when the implant is loose in flexion.
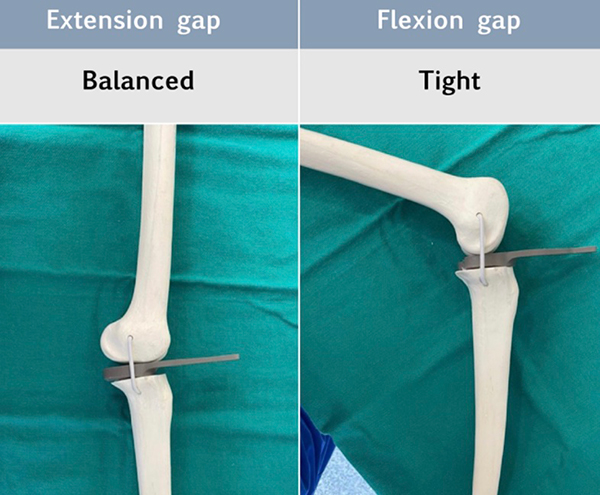
The causes for a stiff knee replacement are multifactorial but may also relate to surgical factors, where the extension and flexion gaps are not balanced. A potential cause of this is when the surgeon places the tibial component too high on the bone, or under-resecting the tibial bone. This in turn leads to a tight knee throughout a range of motion. In order to get the knee to a straightened position, the surgeon has to use a very thin plastic (polyethylene) liner. The knee is then balanced in extension but stiff in flexion. A stiff knee replacement can be very dissatisfying for the patient, leading to further surgery (“manipulation under anesthesia”), prolonged and painful rehabilitation, and in severe cases, revision replacement.
Pataller maltracking and misalignment of the knee can be subtle but are among the causes of pain at the front of the knee following knee replacement(3). Pain can be caused by increased pressure in the patellofemoral section of the knee, or when the components are placed in such a way as to cause a pull of the patella laterally, such as when the implants are placed in a “valgus” orientation(3). When the components are placed in a way as to “overstuff” the patella, pain can result from the increased contact pressure in and around the kneecap. These patellar disorders and misalignment problems can largely be prevented and are predictably avoiding with the use of robotic surgery, below.

The best way to guarantee a pain-free knee replacement is to ensure that the implants are aligned as perfectly as possible during the initial replacement, generating full motion immediately with balanced stability. This can in large part be improved with the use of robotic-arm assisted technology. The benefits of robotic surgery are that there is a 3-dimensional plan with sub-millimeter precision with where the implants will be positioned before the procedure even starts. This plan can then be modified during surgery depending on the balance and reactivity of the patient’s ligaments and soft tissues. We are continuing to observe the benefits of robotic technology in knee replacement which is making important strides in eliminating the possibility of dissatisfaction following surgery.
If you are concerned about long-term comfort following surgery, Dr. Thomas Obermeyer can provide expert insights on How to Prevent Chronic Pain After Knee Replacement. Through the use of modern anesthetic techniques and precise implant alignment, Dr. Obermeyer aims to deliver a pain-free, functional result. He sees patients at his offices in Schaumburg, Bartlett, and Elk Grove Village, Illinois, and treats individuals from throughout Hoffman Estates, Palatine, Elgin, Streamwood, Arlington Heights, and Roselle.
References
- American Joint Replacement Registry (AJRR): 2023 Annual Report. Rosemont, IL: American Academy of Orthopaedic Surgeons (AAOS), 2023
- Thiele K, Perka C, Matziolis G, Mayr HO, Sostheim M, Hube R. Current failure mechanisms after knee arthroplasty have changed: polyethylene wear is less common in revision surgery. J Bone Joint Surg Am. 2015 May 6;97(9):715-20. doi: 10.2106/JBJS.M.01534. PMID: 25948517.
- Assiotis A, To K, Morgan-Jones R, Pengas IP, Khan W. Patellar complications following total knee arthroplasty: a review of the current literature. Eur J Orthop Surg Traumatol. 2019 Dec;29(8):1605-1615. doi: 10.1007/s00590-019-02499-z. Epub 2019 Jul 13. PMID: 31302764.
At a Glance
Dr. Thomas Obermeyer
- 15+ years of training and experience treating complex shoulder and sports medicine conditions
- Expert subspecialized and board-certified orthopedic care
- Award-winning outstanding patient satisfaction scores
- Learn more
